Article Text

Abstract
Objective The effect of fall prevention exercise programmes in residential aged care (RAC) is uncertain. This paper reports on an intervention component analysis (ICA) of randomised controlled trials (RCTs), from an update of a Cochrane review, to develop a theory of features of successful fall prevention exercise in RAC.
Methods Trial characteristics were extracted from RCTs testing exercise interventions in RAC identified from an update of a Cochrane review to December 2022 (n=32). Eligible trials included RCTs or cluster RCTs in RAC, focusing on participants aged 65 or older, assessing fall outcomes with stand-alone exercise interventions. ICA was conducted on trials with >30 participants per treatment arm compared with control (n=17). Two authors coded trialists’ perceptions on intervention features that may have contributed to the observed effect on falls. Inductive thematic analysis was used to identify the key differences between the trials which might account for positive and negative outcomes.
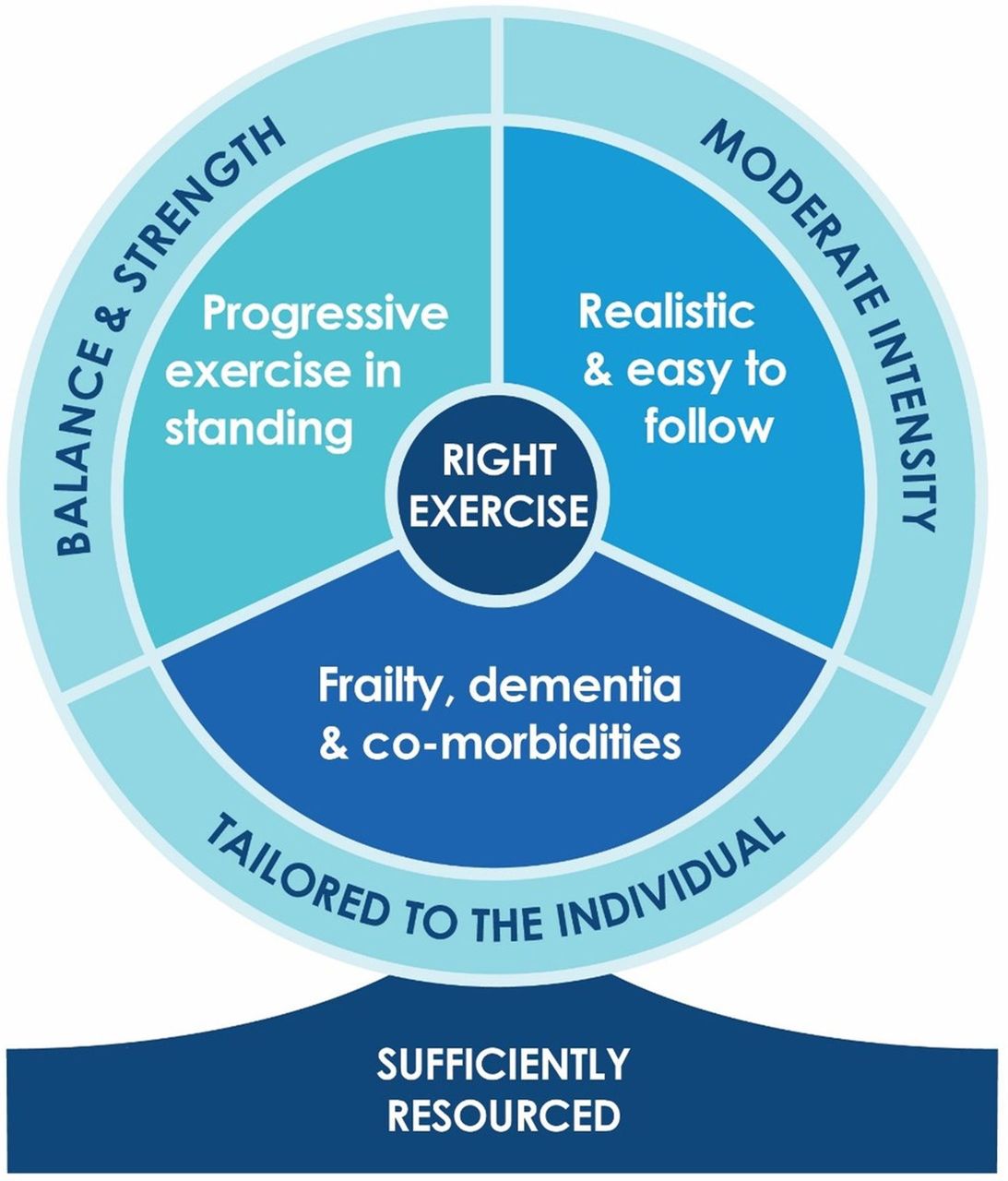
Results 32 RCTs involving 3960 residents including people with cognitive (57%) and mobility (41%) impairments were included. ICA on the 17 eligible RCTs informed the development of a theory that (1) effective fall prevention exercise delivers the right exercise by specifically targeting balance and strength, tailored to the individual and delivered simply at a moderate intensity and (2) successful implementation needs to be sufficiently resourced to deliver structured and supervised exercise at an adequate dose.
Conclusions This analysis suggests that delivering the right exercise, sufficiently resourced, is important for preventing falls in RAC. This clinical guidance requires confirmation in larger trials.
- Exercise
- Accidental Falls
- Aged
- Qualitative Research
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request. Proposals for data should be directed to the corresponding author (rik.dawson@sydney.edu.au).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Exercise reduces the risk of falls for older people in the community with tailored balance and functional exercise having the strongest fall prevention effect.
The evidence concerning the effects of fall prevention exercise in residential aged care (RAC) is less clear, limiting guidance for clinicians working in RAC.
WHAT THIS STUDY ADDS
This intervention component analysis (ICA) used a mixed method approach to develop a theory of potential features of effective fall prevention exercise in RAC that can be explored and validated in future analyses. This theory indicates that (1) exercise interventions for fall prevention in RAC should include balance and strength exercise delivered at a moderate intensity and tailored to the individual and (2) exercise programmes in RAC are more likely to be successful if structured, supervised and resourced to deliver an adequate dose.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Findings from this ICA will assist implementation of fall prevention programmes in RAC; guide a qualitative comparative analysis and subgroup meta-analysis in RAC and inform the design of interventions to be tested in future large clinical trials in RAC.
Introduction
Falls are prevalent in residential aged care (RAC), affecting half of residents annually, diminishing independence, increasing care burden and imposing economic costs.1 2 Implementing effective interventions holds the potential to benefit older individuals and alleviate healthcare burden.3
The 2019 Cochrane Review in community-dwelling older adults reported exercise prevents falls, particularly with balance and functional exercises, reducing rates by 24% (rate ratio (RaR) 0.76, 95% CI 0.70 to 0.81; 7920 participants, 39 studies; I2=29%, high-certainty evidence).4 Programmes combining balance, functional and resistance exercises reduced the rate of falls by 34% (RaR 0.66, 95% CI 0.50 to 0.88; 1374 participants, 11 studies; I2=65%, moderate-certainty evidence). Conversely, the 2018 Cochrane Review for residents in aged care reported uncertain effects of exercise on falls (RaR=0.93, 95% CI 0.72 to 1.20; 2002 participants, 10 studies; I2=76%, very low-quality evidence).5 Subgroup analyses couldn't explain high outcome heterogeneity, challenging clinicians in selecting effective exercise programmes.6
In this study, we conducted an intervention component analysis (ICA), a method utilising inductive qualitative analysis to collate trialists’ reflections on the factors influencing the success or failure of an intervention. Our objective is to answer three research questions. (1) What are the characteristics of trials included in the updated Cochrane Review?5 (2) Using ICA, what are the intervention and implementation features that are present in successful fall prevention exercise programmes in RAC? and (3) What explanatory theory does the information in the first two questions suggest for supporting knowledge translation of fall prevention programmes and informing future research in RAC?7
Methods
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.8 This ICA was developed according to the methodology detailed in an existing published theory.7
Selection of studies
Criteria followed Cameron et al’s 2018 Cochrane Review on preventing falls in older care facility residents.5 New trials from 2017 to December 2022 were sourced from CENTRAL, MEDLINE, Embase and CINAHL databases, adhering to the Cochrane Review’s search methods.5 Only randomised controlled trials (RCTs) and cluster RCTs with participants aged 65+ in RAC, reporting fall rates or risk and comparing exercise interventions to usual care or control were considered. Trials with ≥30 participants per arm were included to mitigate small sample bias,9 encompassing outcomes that reduced, had no effect neutral, or increased falls (figure 1).

PRISMA flowchart of trial selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data extraction
Trial features
Two aged care physiotherapists (RD and WK) extracted trial and participant characteristics (trial design, sample size, age, gender, cognitive and mobility status), exercise features (type, duration, dose, delivery, supervision, tailoring, intensity) and fall outcomes from new trial’s final endpoint or the Cochrane Review.5 Adherence was classified as good if the participant exercise session attendance rate exceeded 50%, and/or if 75% or more of the participants attended 50% or more of the exercise sessions.10 Exercise classifications adhered to the Prevention of Falls Network Europe (ProFANE) exercise taxonomy11 and include standardised intensity ratings like the Borg Rating of Perceived Exertion Scale12 and trialist’s self-classification. Low-intensity exercise refers to gentle physical activity where the heart rate and breathing are low; moderate-intensity exercise elevates heart rate and breathing moderately; while high-intensity exercise elevates heart rate and breathing to near maximal effort, making it difficult to sustain a conversation.12 The ProFANE group’s exercise descriptors cover structured programmes including strength exercises (resistance training with weights and/or body weight), gait, balance and functional exercises mirroring daily movements (eg, stepping, sit-to-stand), flexibility, general physical activity and 3D exercises like Tai Chi. Disagreements were resolved through discussion and involvement of a third author as required (SD and JS).
Fall outcomes were expressed as rate or risk ratio with 95% CI. They were coded positive (<0.75), neutral (0.75 to 1.25) or negative (>1.25) based on Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) group guidance for consideration of ‘appreciable benefit or harm’.13 Data analysed in Excel.
Trial quality
Two trained independent physiotherapists (RD, WK) assessed study quality using the Physiotherapy Evidence Database (PEDro) scale, which evaluates 11 criteria: inclusion criteria, random allocation, concealed allocation, baseline similarity, blinding of subjects, therapists and assessors, completeness of follow-up, intention-to-treat analysis, between-group statistical comparisons and outcome measures.14 Disagreements were resolved through discussion. External validity, the first item, does not contribute to the score, yielding scores from 0 to 10. Ratings: 0–4 (poor), 4–5 (fair) and 6–8 (good). Scores of 9–10 (excellent) are n't feasible in exercise trials due to blinding constraints.
Intervention component analysis
We conducted ICA over four stages:
Authors (RD and WK) described the trial features, quality and classified fall outcomes in Excel.13
Authors (RD and JS) coded trialists’ reflections on effective and ineffective features in eligible publications’ discussion and conclusion sections, including any additional trial-related documents (eg, protocols, process evaluations) identified through systematic search, pearling and hand searching. A selection of publications was coded independently in duplicate; the remainder were extracted by RD and checked by JS, with disagreements resolved through discussion. Codes were stored in NVivo V.12.15
RD conducted an inductive thematic analysis in NVivo on included trials, grouping codes to develop themes and subthemes on successful intervention features and implementation.16 JS and SD reviewed groupings to ensure thematic agreement. Both JS and SD experienced qualitative and falls researchers, respectively, offered critical perspectives to the thematic analysis as non-exercise professionals.
RD reviewed the themes against the trial outcomes and the intervention features to develop a theory regarding the types of intervention features and implementation strategies most likely to be effective in preventing falls in RAC. All authors were involved with developing the final theory.
Equity, diversity and inclusion statement
The author group consists of junior, mid-career and senior researchers from different countries and disciplines, most of whom are women. Our study population included both male and female older adults from different socioeconomic and geographical backgrounds.
Results
Trial and participant characteristics from an updated systematic review
Thirty-two trials were included across 16 countries involving 3960 participants with 35 exercise intervention arms. Many trials have small sample sizes, with a median number of 71 participants and a range from 1617 to 682 participants.18 Participant ages ranged from 6819 to 92 years,20 21 with a median of 82 years; 74% were women. Eighteen (57%) trials included people with cognitive impairment and 13 (41%) trials included those with mobility disabilities. Trial length varied from 4 weeks22 to 104 weeks,23 with a median of 12 weeks (IQR 12–26). Total intervention hours ranged from 1.5 hours24 to 112 hours,25 with a median trial dose of 22 hours (IQR 14–36) or 1.8 hours per week, comprising a median of three sessions per week (IQR 2–3) with a median session duration of 33 min (IQR 25–48). Sixteen (52%) trials met good exercise adherence criteria. Ten (32%) trials reported adverse events, including two falls during exercise.26 27 Most trials compared an exercise intervention with usual care, defined as seated low-intensity range of movement exercise programmes, self-directed or social programmes (online supplemental material A).
Supplemental material
Intervention components
The most common exercise intervention was gait, balance and functional training combined with strength training in 18 (51%) intervention arms. The most common single intervention was gait, balance and functional training in five (14%) arms. In 20 (63%) trials, exercise interventions were tailored to the individual. Fifteen (47%) trials delivered exercise at moderate intensity, 14 (44%) at low intensity and three (9%) at high intensity. Thirteen (41%) trials were led by physiotherapists, three (9%) by other health professionals and trained non-exercise professionals led 14 (44%) trials; five trials (16%) did not report who led the intervention. There was a mix of supervised and unsupervised individual and group exercise, with supervised groups being the most common in 19 trials (59%) with a median of five participants per group (IQR 5–8) (online supplemental material B)
Supplemental material
Quality assessment
The PEDro study quality summary is displayed in online supplemental material C. The median PEDro quality score for the trials included in the ICA was ‘good’ (6/10).
Supplemental material
Intervention component analysis
The ICA included 17 trials involving 3293 participants with a median age of 82 years (ranging from 75 to 86 years); 73% were female participants. Ten trials (59%) included people with cognitive impairment and seven trials (41%) included people with mobility disability (table 1). The participant characteristics of the ICA trials reflected the 32 trials included in the updated Cochrane review. ICA identified two major themes related to exercise features and implementation, each with three subthemes (table 2). ICA Codebook outlines the coding framework, which is displayed in online supplemental material D. The correspondence between the themes and the trial’s effectiveness synthesis are summarised in table 3. The ICA also identified some study design features that could be associated with intervention effects.
Supplemental material
Summary characteristics of 17 ICA trials at inclusion
Development of intervention and implementation themes in the ICA
Presence of themes and subthemes in ICA trials (effectiveness synthesis)
The right exercise
The most common theme supported by the trialist’s commentary focused on providing the right exercise to reduce falls. The results of our thematic analysis suggest that the right exercise is a combination of exercise that targets balance and strength, tailored to the individual’s physical and cognitive comorbidities and delivers moderate-intensity exercise (table 2). Ten trials targeted progressive standing balance and strength exercise,27–36 12 studies delivered tailored exercise prescription18 27–35 37 38 and 6 studies delivered moderate-intensity exercise subtheme27–32 (table 2). Six of eight effective trials27–32 supported the right exercise theme, while zero out of nine neutral or negative trials did not (table 3).
Supporting exercise engagement
The second theme centred on supporting exercise engagement. However, there was less trialist commentary on this theme (table 2) and only two of eight effective trials included all the subthemes.27 31 Only the first subtheme had sufficient evidence to progress to the ICA theory (table 3). Four of eight effective trials provided sufficient resourcing as defined as trials that delivered structured and supervised exercise at a dose greater than 30 hours27 28 30 32 compared with two of nine neutral or negative trials.34 38 Group exercise that offers socialisation opportunities were offered in five of eight effective trials27 28 30–32 but was also offered in four of nine neutral or ineffective trials.33 34 36 38 Fall prevention education was a feature in three of eight effective trials27 29 31 and one of nine neutral or negative trials.23 The effectiveness synthesis demonstrated that there was insufficient evidence to involve the group exercise and fall education subthemes in the final ICA theory displayed in figure 2.

{kind=link}
{kind=link}
ICA theory of effective fall prevention exercise in residential aged care. ICA, intervention component analysis.
Trial methodological design features
Two features emerged as themes relating to trial design and their impact on effective fall prevention trials. Seven authors commented that some trials are too small to detect significant changes in falls.23 28 30 33 34 36 38 Five authors commented that trial designs that involved an active control diluted the fall effect.30–33 36
Discussion
ICA is a valuable tool for researchers, clinicians and policymakers, enabling the identification of promising intervention components and their implementation strategies. Through ICA methodology, trialist perspectives are plotted against trial outcomes, culminating in the development a theory of effectiveness that can be explored and validated though subsequent analyses. This ICA theory indicates that effective fall prevention programmes within RAC centre on the delivery of the right exercise when sufficiently resourced. However, larger trials are required to expand the evidence base for effective fall prevention exercise programmes in RAC.
In this ICA, we propose that right exercise is tailored, moderate intensity, balance and strength exercise. In general, this is in accordance with the evidence for effective exercise programmes in the community.4 However, Sherrington and colleagues’ subgroup analysis revealed that balance and functional exercises with or without resistance exercises had the greatest fall prevention effects in the community.4 ,5 Cameron and colleagues’ subgroup analysis for combination exercises in RAC, including balance and strength exercise30 32 33 35 38 or physical activity plus strength,17 did not find a significant reduction in falls (RaR 0.94, 95% CI 0.6 to 1.47); however, there were only six trials in this subgroup analysis.5 Our ICA was based on an update of Cameron et al’s Cochrane review, which reported that balance and strength exercises were the most prescribed interventions in effective trials (88%) compared with those with neutral or negative fall outcomes (33%). Becker and colleagues’ multifactorial trial in RAC also supports this finding. They reported that progressive standing balance and strength exercises reduced the rate of falls by 45%.39
Our review of trial characteristics revealed that 20 out of the 32 trials were tailored to the individual. In the ICA, 88% of positive trials tailored the exercise programmes compared with 56% of trials with neutral or negative fall outcomes. Several trialists stated that exercise needs to be tailored throughout the programme to cater for participants’ changing physical and cognitive capabilities to learn the programme and to maintain exercise adherence, which is a key factor in reducing falls.33 35 38 40 Contrary to this finding, a recent review of tailored exercise delivered in the community found no significant reduction in fall outcomes.41
Six effective trials delivered exercise at a moderate intensity27–32 compared with two effective trials that delivered exercise at a low intensity.37 40 Among the trials with neutral or negative fall outcomes, both low or high intensity models were tested. Kerse et al revealed that low-intensity exercise delivered in small doses throughout the day by care workers as part of the resident’s usual activities was ineffective.18 Faber et al reported that high-intensity individual training was neither effective nor sustainable for long-term exercise due to the resident’s high level of comorbidities.38 Nowalk, Yokoi and Sakamoto and colleagues all commented that successful exercise interventions should be delivered in a way that is simple and easy to learn to maximise exercise compliance in RAC and increase exercise intensity over time.23 40 42
Trialists provided limited comments on ideal implementation strategies. However, the ICA suggested the importance of adequate resources to support exercise structure, supervision and dosage. Analysis of trial characteristics revealed a median weekly dose of 1.8 hours across 32 trials from this updated Cochrane search, significantly lower than the 3 hours/week recommended by Sherrington et al’s meta-regression for effective community-based fall prevention.43 Kerse et al emphasised the need for funding to support more intensive interventions and supervision,18 while Kovacs et al stressed the importance of sufficient physiotherapy resources for effective fall prevention exercise.32 More research is required to better understand the implementation of an ideal fall prevention exercise programme in RAC. However, there is likely a higher need for supervision in this setting, given the high level of frailty and comorbidities in this population.
This ICA suggests future RCTs on fall prevention exercises in RAC should increase their sample size, enhance study quality by reducing bias in the design and improve reporting. A total PEDro score of 8 is optimal for multifaceted interventions like exercise trials, contrasting with the median trial score of 6.44 In the 32 trials identified in the Cochrane review update, 15 enrolled fewer than 60 participants, requiring a larger sample size to detect differences in fall rates.9 Additionally, many trials did not meet the standards of the Consolidated Standards of Reporting Trials (CONSORT) statement.45 The reporting of almost two-thirds of trials did not describe allocation concealment, with some not clearly describing their control group. This poor reporting made coding exercise features difficult and reduces the generalisability of this ICA.
Hewitt et al’s Sunbeam trial achieved an optimal PEDro score of 8,27 demonstrating effective fall prevention through a physiotherapy-led tailored, progressive standing balance and strength exercises. With a 55% fall rate reduction and improved mobility outcomes, the trial implemented exercise engagement supports detailed in our thematic analysis (table 3). It provided a mean exercise dose of 36 hours, employing user-friendly electronic equipment, fostering high programme adherence via staff and resident education and supervised group exercise for socialisation. Similarly, the Otago Exercise Program, known for its balance and strength focus, demonstrated effectiveness in community settings and merits investigation in RAC.46
Research implications
The ICA theory will inform a qualitative comparative analysis (QCA), which examines the ICA theory’s consistency and identifies conditions contributing to effective falls prevention programmes.7 While both ICA and QCA facilitate identifying processes and potential mechanisms that link intervention features and outcomes, we acknowledge that causation cannot be definitively established using probabilistic or counterfactual accounts using these approaches. A recent study employing ICA and QCA methodologies on multifactorial fall prevention interventions highlighted the importance of incorporating exercise and engaging aged care staff and managers in implementing tailored strategies in RAC.47 These findings emphasise the need for future research to explore multifactorial interventions in RAC settings, explore specific programme needs for recurrent fallers who may have different needs compared with single fallers and in other settings to enhance the generalisability of our ICA and bolster the quality of evidence.
To enhance reporting, future trials should adhere to recognised trial reporting guidelines such as the CONSORT statement,45 Standard Protocol Items: Recommendations for Interventional Trials statement,48 Template for Intervention Description and Replication checklist49 and Consensus on Exercise Reporting guidelines50 to enhance reporting.
Strengths and Limitations
This updated systematic review, incorporating ICA, ensures rigorous methodology. Nonetheless, limitations include the exclusion of conference abstracts, trial records and studies on exercise within multifactorial interventions. Some trials excluded older adults with high cognitive and mobility impairments, potentially limiting result generalisability. Additionally, exercise descriptions were often broad, lacking specificity like sensorimotor training. Incomplete reporting may have compromised ICA quality, hindering a more comprehensive explanatory theory.
Conclusion
Examining trial characteristics in the updated Cochrane Review on fall prevention exercise in RAC reveals intervention heterogeneity. This ICA enriches trial descriptors, aiding theory development and practical applications. Trialists suggest sufficiently resourced, tailored balance and strength exercises delivered at moderate intensity may prevent falls. Future larger trials should scrutinise this ICA theory, delivery mode, dose, different implementation and engagement strategies, and adhere to reporting guidelines.
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request. Proposals for data should be directed to the corresponding author (rik.dawson@sydney.edu.au).
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @dawson_rik, @CathieSherr, @venisakwok, @mabpinheiro, @SuzanneMDyer
Contributors All authors conceptualised and designed the study and were involved in applying the ICA methodology in this study. Analysis of data was undertaken by RD, WSK, JS and SD. RD drafted the manuscript. RD is the guarantor and has access to the data, accepts full responsibility for the conduct of the study and controlled the decision to publish. All authors critically revised the manuscript for intellectual content, approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The National Health and Medical Research Council (NHMRC) of Australia funded Centre for Research Excellence – Prevention of Fall related Injuries provides RD and WK with PhD scholarship funding, and JS and SD partial salary funding. MP receives salary funding from an NHMRC Fellowship.
Disclaimer This manuscript is based on Chapter Three of RD’s thesis by publication called 'Telehealth Physiotherapy to Deliver Exercise in Aged Care Settings' which was submitted to the University of Sydney 14 March 2024. The funding organisations listed above did not have a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.