Article Text

Abstract
Objective To examine the relationship between postpartum physical activity and maternal postnatal cardiometabolic health, breastfeeding, injury, and infant growth and development.
Design Systematic review with random-effects meta-analysis and meta-regression.
Data sources Eight online databases were searched up until 12 January 2024.
Eligibility criteria Studies of all designs in all languages were eligible (except case studies and reviews) if they contained information on the population (postpartum people), intervention (frequency, intensity, duration, volume, or type of exercise, alone (‘exercise-only’) or in combination with other intervention components (eg, dietary; ‘exercise+co-intervention’), comparator (no or low volumes of physical activity), and outcomes: hypertension, diabetes, cardiometabolic risk factors (systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol, high density lipoproteins, low density lipoproteins, and triglycerides, glycated hemoglobin (HbA1C), glucose and insulin concentration), breastfeeding (breast milk quality and volume), infant growth (length and weight) and development, or postpartum injury.
Results 46 unique studies (n=8766 participants) from 20 countries were included. Moderate certainty of evidence showed exercise+co-interventions reduced the odds of developing diabetes by 28% (7 randomised controlled trials (RCTs), n=2496; OR 0.72 95% CI 0.54, 0.98, I2 12%), reduced SBP (10 RCTs, n=2753; mean difference (MD) −2.15 95% CI −3.89 to –0.40, I2 73%) and DBP (9 RCTs, n=2575; MD −1.38 95% CI −2.60 to –0.15, I2 66%) compared with controls. Infant growth and development, breast milk quality and quantity, and risk of injury were not different between exercise and control groups.
Conclusions Physical activity improves cardiometabolic health without adversely impacting breast milk supply or quality, infant growth or maternal injury.
- Exercise
- Diabetes
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN
Postpartum women and people are at increased risk of developing diabetes and cardiovascular disease if they have experienced pregnancy complications such as pre-eclampsia and gestational diabetes.
The postpartum period is critical for the implementation of preventative measures to reduce chronic disease risk. Physical activity has been proposed as a promising intervention but the impact on chronic disease risk following childbirth is poorly understood.
Concerns persist about whether postpartum physical activity increases the risk of injury, or could impair breast milk supply and quality, and subsequently infant growth and development.
WHAT ARE THE NEW FINDINGS
Maternal physical activity reduces the risk of developing type 2 diabetes by 28% and reduces blood pressure after childbirth.
Postpartum physical activity did not alter breast milk quality and supply, infant growth and development, or the risk of injury.
Introduction
Over the last decade, the importance of maternal and infant health during pregnancy and postpartum has been prominent in medical and public thinking. This unique period is now believed to be a critical window of opportunity to identify people at high risk for future chronic disease and to implement early interventions to improve the lifelong health of both mother and infant. In 2011, the American Heart Association listed pregnancy complications (including pre-eclampsia, gestational hypertension and gestational diabetes mellitus (GDM)) as risk factors as strong as smoking for development of cardiovascular disease following pregnancy.1 Those who have experienced complications in pregnancy have an elevated risk for future cardiometabolic diseases. GDM increases the odds of cardiovascular disease (OR 1.68), hypertension (HR 1.54) and metabolic syndrome (HR 2.51).2 3 Up to 70% of those diagnosed with GDM will subsequently develop type 2 diabetes, with a nearly 10-fold increased risk of diagnosis in the first 5 years after delivery compared to those without GDM.4 5 Hypertensive disorders of pregnancy increase the odds of cardiovascular disease (OR 1.67), stroke (OR 1.83) and hypertension (OR 3.13).2 The most sobering statistic is that those who develop pre-eclampsia are at increased risk of death from cardiovascular disease (HR 2.14) in the first decade after delivery.6 While the physiological ‘stress test’ of pregnancy identifies those at high risk, the postpartum period is critical to implementing preventive measures for future chronic disease. In this respect, a 2021 Scientific Statement From the American Heart Association identified that practising physical activity during the postpartum period and beyond is a key intervention to decrease future cardiovascular disease risk following the development of pregnancy complications.2
While the aetiology of cardiovascular disease and diabetes is complex, breastfeeding has emerged as a potential modifiable factor that could influence the risk of cardiometabolic diseases in the mother later in life. It has been suggested that breastfeeding may have a beneficial impact on risk factors for cardiometabolic diseases including hypertension, dyslipidaemia and insulin resistance thereby reducing the risk of future cardiovascular disease and type 2 diabetes following pregnancy.7 8 Breastfeeding is also a fundamental aspect of infant health, as it provides the requisite energy and nutrients for growth and development, as well as antibodies which protect against common childhood illnesses.9
While postnatal physical activity and breastfeeding are of particular importance for the future health of the mother and her child, the impact of postnatal physical activity on breastfeeding and on infant growth and development, as well as on maternal injury, is not well understood. It has been suggested that the timing and intensity of returning to physical activity or sport, as well as breastfeeding, may predispose those in the postpartum period to injury.10 It is understood that postpartum injuries occur in soft, hard and neural tissues, primarily affect the trunk region, and there are a multitude of factors influencing risk of injury.11–15 However, there is a lack of consensus and under-reporting of injury data to determine the dose-response relationship of physical activity and injury incidence and severity in the postpartum period.
This systematic review and meta-analysis is part of a series of reviews which will form the evidence base for the Canadian Society for Exercise Physiology 2025 Canadian Guideline for Physical Activity, Sedentary Behaviour and Sleep throughout the First Year Postpartum (hereafter referred to as the Guidelines). The purpose of this systematic review and meta-analysis was to examine the relationships of postpartum physical activity on cardiometabolic risk factors, breastfeeding, infant growth and development, and maternal injury.
Methods
In April 2022, the Guideline Consensus Panel was formed and met to identify key health outcomes for the Guideline development. The panel included researchers, methodological experts and representatives from the Society for Obstetricians and Gynaecologists of Canada, Canadian Society for Exercise Physiology, College of Family Physicians of Canada, Canadian Physiotherapy Association, Canadian Association of Midwives, and Canadian Academy of Sport and Exercise Medicine. Patient preferences were obtained via online survey to inform these decisions but were otherwise not involved in the project. During this meeting, 21 outcomes were identified including 10 ‘critical’ maternal health outcomes, 9 ‘important’ maternal health outcomes, and 2 ‘important’ infant health outcomes in relation to postpartum maternal health behaviours (physical activity, sedentary behaviour and sleep).16 17 Hypertension, diabetes, cardiometabolic risk factors, breastfeeding and injury, were identified as ‘critical’ outcomes while infant growth (ie, infant length and weight) and development were identified as ‘important’ outcomes.
The current systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18 The completed PRISMA checklist is included in the online supplemental file.
Supplemental material
Study protocol and registration
The protocol was registered with PROSPSERO, the International Prospective Register of Systematic Reviews, on 20 September 2022 (registration number CRD42022359282; available from: www.crd.york.ac.uk/prospero/display_record.php?RecordID=359282). Ethics approval was not required.
Eligibility criteria
The PICOS (population, intervention, comparison, outcome, study design) framework19 was used to guide this review.
Population
The population of interest was women and people in the first year following childbirth. In cases where a study recruited participants beyond 12 months after delivery, the study was included only if the majority of participants were in their first year postpartum.
Intervention/exposure
The intervention was subjective or objective measures of prescribed exercise frequency, intensity, duration, volume, duration or type. Although exercise is a subtype of physical activity, for the purpose of the current review, we used these terms interchangeably. Accordingly, exercise and physical activity were defined as any bodily movement generated by skeletal muscles that results in energy expenditure above resting levels.20 21 Interventions including exercise alone (termed ‘exercise-only interventions’) or in combination with other interventions (such as diet, termed ‘exercise+co-interventions’) were considered. Studies were included if the physical activity/exercise intervention was initiated in the first year postpartum. Interventions which began during pregnancy were included if the majority of the intervention continued following childbirth.
Comparison
Eligible comparators were no intervention, minimal contact (ie, online intervention), standard care (education only, standard medical care for those in the postpartum period, author defined) and active controls (ie, low intensity exercise).
Outcomes
Relevant outcomes were chronic breastfeeding (breast milk volume and composition), hypertension, diabetes, and cardiometabolic risk factors (systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol, high density lipoproteins, low density lipoproteins, and triglycerides, HbA1C, glucose and insulin levels (fasted or 1 hour and/or 2 hours after an oral glucose tolerance test)), postpartum injury, infant growth (length and weight), and development.
Study design
Primary and grey literature of any study design were eligible with the exception of review articles, case studies and non-original research.
Additional considerations
Eligible studies were not limited by publication language or date. Studies not published in English or French were initially translated using Google translate to determine eligibility for inclusion. If selected for extraction, they were analysed with the assistance of a native speaker.
Information sources
A comprehensive search was created and run by a research librarian in the following databases: MEDLINE, EMBASE, CINAHL, SPORTDiscuss, Evidence-Based Medicine Reviews (Ovid), Scopus, Web of Science, and ClinicalTrials.gov up to 17 August 2022. An updated search of these databases was performed on 12 January 2024. Collaborator-nominated papers were accepted for consideration. Reference lists of included studies and relevant reviews were screened for additional, relevant papers. Complete search strategies are presented in the online supplemental file.
Supplemental material
Study selection and data extraction
Search results were uploaded to Covidence (Melbourne, Victoria, Australia), an online systematic review management software, where duplicate records were removed. Titles and abstracts of all unique articles were independently assessed by two reviewers. Full-text articles of titles and abstracts meeting initial screening criteria were retrieved. Two independent reviewers then examined all full-text articles for inclusion, with disagreements resolved through discussion between reviewers or a third reviewer if needed.
Two reviewers independently extracted data from all included studies into Google Sheets (Google, Mountain View, California, USA). Two content experts independently verified the extracted data. For each individual study, the most recent or complete version of the publication was selected as the ‘parent’ paper; however, relevant data from all publications related to each unique study were extracted.
Extracted data included study characteristics (eg, year, study design, country), population characteristics (eg, number of participants, age, prepregnancy body mass index, previous physical activity levels, parity and pregnancy complications), intervention (prescribed exercise frequency, intensity, duration, volume, type, duration of intervention), comparators (no exercise or different types of exercise), co-intervention type and outcomes. If data were not available for extraction, study authors were contacted for additional information.
Certainty of evidence assessment
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework was used to assess the certainty of evidence across included studies for each anthropometric outcome and study design (randomised controlled trial (RCT) and superiority RCT).22 Accordingly, evidence from RCTs was considered ‘high’ quality and was graded down if there was a concern with risk of bias (ROB),23 indirectness,24 inconsistency,25 imprecision26 or risk of publication bias,27 because these factors reduce the level of confidence in the observed effects. Evidence from all non-randomised interventions and observational studies began with a ‘low’ quality rating and, if there was no cause to downgrade, was upgraded if applicable according to the GRADE criteria (eg, large magnitude of effect, evidence of dose-response).28
Two reviewers independently and systematically assessed ROB of included studies at the individual study level with a modified Joanna Briggs Institute (JBI) Manual for Evidence Synthesis.29 The ROB in RCTs was assessed using the standardised critical appraisal instruments from the JBI Critical Appraisal of Evidence Effectiveness tool.30 The JBI checklist was used to determine the extent to which a study had addressed the possibility of bias in its design, conduct and analysis. Specifically, all studies were screened for potential sources of bias, including inappropriate sampling, flawed measurement of exposure, flawed measurement of outcomes, selective/incomplete outcomes, unidentified confounding factors, and inappropriate statistical analysis. In case of rating differences, discrepancies were resolved through discussion. The overall ROB of a study was defined as high risk when more than a third of the factors (RCTs: ≥3 of 10 factors; non-RCT: ≥4 of 13 factors; cross-sectional studies: ≥3 of 9 factors; cohort studies: ≥4 of 13 factors) were marked as high risk. The ROB across studies was considered ‘serious’ when studies with the greatest influence on the pooled result (assessed using weight (%) given in forest plots) presented with high ROB. The greatest influence on the pooled result was determined as follows: the studies that had the greatest individual % contribution in the meta-analyses, when taken together, contributed to >50% of the weight of the pooled estimate.
Inconsistency across studies was assessed using both statistical tests and visual inspection of forest plots.31 The Cochran’s Q (α=0.05) was used to detect statistical heterogeneity and I² statistic was employed to quantify the magnitude of statistical heterogeneity between studies. In the case where high statistical heterogeneity (I²>50%) was observed, the evidence was considered for downgrading if the direction of effect was inconsistent across most studies, with minimal overlap of CIs, and if such heterogeneity remained unexplained after conducting meta-regression and/or subgroup analyses. Indirectness was considered serious when PICOS criteria differed substantially across studies. Imprecision was considered serious or very serious when the sample size was small (<300 in each arm or <100 in each arm, respectively) and/or when the effect estimate was imprecise with a wide CI including the no effect value (does not rule out a small harm or negative effect).32 Publication bias was assessed when there were at least 10 studies included in the meta-analysis. Otherwise, it was deemed non-estimable and not rated down.
Statistical analysis
Meta-analyses were conducted for each outcome using ReviewManager (RevMan) V.5.4 (Cochrane, London, the UK). Either the mean difference (MD) or the standardised mean difference (SMD) in change scores (preintervention to postintervention) was calculated when appropriate for continuous outcomes. SMD effect sizes were calculated using Hedges’ g. Continuous outcome analyses was conducted using DerSimonian and Larid random-effects models with an inverse-variance approach.33 An effect size of 0.2, 0.5 and 0.8 were considered small, moderate and large, respectively.34 ORs were calculated for dichotomous outcomes using postintervention events or percentage data. Dichotomous outcome analyses were conducted with a Mantel-Haenszel random-effects method. Statistical significance was defined as p<0.05.
Sensitivity analyses were performed to evaluate whether the observed effects were different when examining the impact of exercise-only versus exercise+co-interventions on the outcomes. When possible, the following a priori subgroup analyses were conducted: (1) When the intervention started (≤12 weeks vs >12 weeks postpartum), (2) Mode of delivery (vaginal vs caesarean section vs mixed), and (3) Type of physical activity (eg, aerobic exercise, resistance training, mixed training, Tai Chi, Pilates, pelvic floor muscle training). If a study did not provide sufficient details to allow it to be grouped into the a priori subgroups, an ‘unclear’ group was created. Additional analyses were conducted to assess whether exercise-only interventions had differential effects based on study time points (ie, immediately postintervention or follow-up time point). Tests for subgroup differences were conducted with statistical significance set at p<0.05. If statistically significant differences were found, subgroup differences were interpreted. The I2 was calculated to indicate the per cent of total variability that was attributable to between-study heterogeneity.
Studies reporting continuous outcomes in other measures of central tendency and/or dispersion (ie, median, range, SE) were converted to mean and SD for analyses.35–37
Equity, diversity and inclusion statement
Our study included all studies (of any designs) on maternal cardiometabolic, breastfeeding, injury, and infant growth and development outcomes with no exclusion criteria on gender, race, ethnicity, sexuality, socioeconomic status, chronic illness or disease. Our research team consisted of 13 individuals from three provinces in Canada and included 12 women and one man from different disciplines, ethnicities and stages across careers. The studies included in this meta-analysis refer to women, but the results are broadly applicable to all postpartum people.
Results
Study selection
The PRISMA flow diagram is presented in figure 1. A comprehensive list of excluded studies is included in the online supplemental file.

The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Study characteristics
Overall, 47 manuscripts reporting on 46 unique studies with 8766 participants from 20 countries were included (32 RCTs,38–71 n=7091; 4 superiority RCTs,72–75 n=275; 4 non-RCTs,76–79 n=120; 3 longitudinal studies,10 80 81 n=1196; 2 cross-sectional studies,82 83 n=84). Among the included interventions, the frequency of exercise ranged from 1 day to 7 days per week and the duration of exercise ranged from 10 min to 60 min per session. The interventions included exercise prescription only, education on physical activity only, or a mix of both. There was a mix of consistent and graded exercise programmes, and some programmes were tailored to each individual participant while others were the same for all participants. The types of exercise included were aerobic (walking, dancing, jogging, cycling), mixed (aerobic+resistance), abdominal, pelvic floor, Pilates, and Tai Chi. Exercise equipment used in the interventions included treadmills, bicycles, stationary bicycles, stability balls, resistance bands, dumbbells, pedometers, yoga mats or no equipment. Exercise accessories included video recordings, and video games (eg, Wii Fit). The exercise programmes were all introduced by a trained exercise professional (eg, physiotherapist, registered dietician, trained nurse, midwife or research assistant) and included a mix of supervised and unsupervised exercise as well as individual-based and group-based training. Interventions were delivered both inperson (eg, at the participants’ homes, hospital gym, community facility) or remotely (via telephone, text messages, email or an online platform such as a website). The interventions began as early as 3 weeks postpartum up until 1 year postpartum. Additional details about included study characteristics can be found in online supplemental tables 1–5 of the online supplemental file.
Certainty of evidence
Overall, the certainty of evidence ranged from ‘very low’ to ‘moderate’ (online supplemental tables 6–16). The most common reason for downgrading the certainty of evidence was imprecision, due to small sample size, that is, lack of power to detect differences with precision, and indirectness (ie, exercise intervention was combined with other intervention, such as nutrition). Publication bias could not be assessed as there were fewer than 10 studies in each forest plot.
Synthesis of data
Randomised controlled trials
Prevalence of diabetes
Overall, there was ‘moderate’ certainty of evidence (downgraded for concerns regarding indirectness) from seven RCTs (n=2469) considering the association between postpartum exercise and the odds of developing diabetes. Overall, postpartum exercise+co-intervention was associated with 28% lower odds of diabetes compared with no exercise (OR 0.72, 95% CI 0.54, 0.98, I2 12%; online supplemental figure 1).
When looking at the maintenance of intervention effect (postintervention to follow-up time point), the pooled summary estimate did not show a reduction for exercise+co-intervention groups as compared with no exercise controls (2 RCTs, n=569; p=0.82, online supplemental figure 3). The overall certainty of this evidence was rated as low and downgraded for concerns regarding indirectness and imprecision. Subgroup analysis on the maintenance of intervention effect was not possible.
Sensitivity analysis
There was only exercise+co-interventions; therefore, sensitivity analysis was not possible.
Subgroup analysis
Stratification of exercise-only RCTs showed no significant difference (timing of the intervention, p=0.15 and type of exercise, p=0.87, figure 2 and online supplemental figure 2) or was not applicable due to insufficient data for subgrouping (mode of delivery).

Effects of postpartum exercise compared with control on the odds of diabetes (randomised controlled trials). The studies were all exercise+co-interventions. Stratified analyses were conducted with studies including when the exercise intervention was initiated early (ie, ≤12 weeks postpartum) or late (ie, >12 weeks postpartum). Analyses were conducted using a random-effects model. CONT, control; df, degrees of freedom; INT, intervention; M-H, Mantel-Haenszel method; PP, postpartum; T2DM, type 2 diabetes.
Fasted glucose
The pooled summary estimate showed no difference between exercise and control for the change in fasted glucose (mmol/L) (12 RCTs, n=2813; MD −0.07, 95% CI −0.25, 0.12, I2 95%; online supplemental figure 7). The overall certainty of this evidence was rated as ‘low’ and downgraded for concerns regarding indirectness and imprecision.
There was no difference in the maintenance of intervention effect on fasted glucose for exercise groups as compared with no exercise controls (5 RCTs, n=740; p=0.18, online supplemental figure 10). The overall certainty of this evidence was rated as ‘low’ and downgraded for concerns regarding indirectness and imprecision.
Sensitivity analysis
The pooled summary estimate for the exercise+co-interventions was not significantly different from the pooled estimate for the exercise-only interventions (p=0.99; online supplemental figure 7). The certainty of evidence was rated as ‘low’ and downgraded for concerns regarding indirectness and imprecision for the exercise+co-interventions and ‘moderate’ regarding imprecision for the exercise-only interventions. Similar results were found for the maintenance of intervention effect on fasted glucose (online supplemental figure 25).
Subgroup analysis
Stratification of exercise-only RCTs by type of exercise showed statistically significant difference in fasted glucose change (p=0.04). One study examining the impact of a Tai Chi intervention demonstrated a greater change in fasted glucose in the exercise group compared with the control (online supplemental figure 9). The certainty of evidence was rated as ‘moderate’ (downgraded for concerns regarding imprecision). The other tests for subgroup differences were either not significantly different (timing of the intervention, p=0.69, online supplemental figure 8) or not applicable due to insufficient data for subgrouping (mode of delivery).
Hypertension prevalence
There were no studies reporting on the effect of postpartum exercise on the odds of hypertension.
Systolic blood pressure
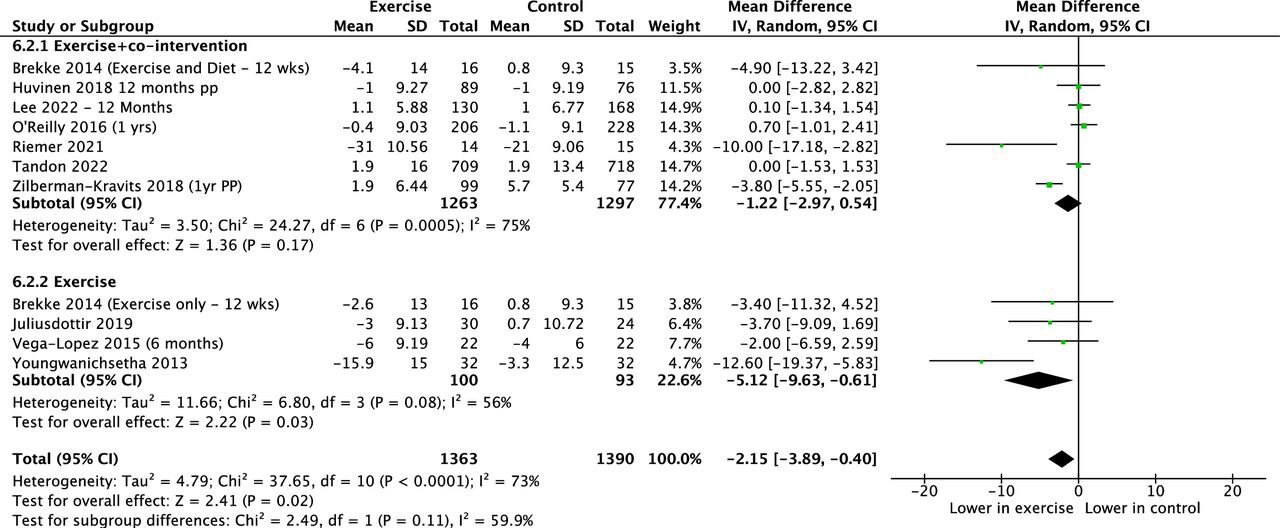
From preintervention to postintervention, the pooled summary estimate showed a greater change in SBP (mm Hg) for exercise groups as compared with the no exercise controls (10 RCTs, n=2753; MD −2.15, 95% CI −3.89 to –0.40, I2 73%; figure 3). The overall certainty of this evidence was rated as ‘low’ and downgraded for concerns regarding inconsistency and indirectness.

Effects of postpartum exercise compared with control on change in systolic blood pressure (mm Hg; randomised controlled trials). Sensitivity analyses were conducted with studies including exercise+co-interventions and exercise-only interventions. Analyses were conducted using a random-effects model. df, degrees of freedom; IV, inverse variance; PP, postpartum.
For the maintenance of intervention effect on SBP, the pooled summary estimate showed no difference during the maintenance phase for exercise groups as compared with the no exercise controls (5 RCTs, n=749; p=0.06; online supplemental figure 50). The overall certainty of this evidence was rated as ‘very low’ and downgraded for concerns regarding inconsistency, indirectness and imprecision.
Sensitivity analysis
The pooled summary estimate for the exercise+co-interventions was not significantly different from the pooled summary estimate for the exercise-only interventions (p=0.11; figure 3). Exercise+co-interventions did not result in a reduction in SBP (7 RCTs, n=2560; MD −1.22, 95% CI −2.97, 0.54, I2 75%). The overall certainty of this evidence was rated as ‘very low’ and downgraded for concerns regarding inconsistency, indirectness and imprecision. Exercise-only interventions resulted in a decrease in SBP (4 RCTs, n=193; MD −5.12, 95% CI −9.63 to –0.61, I2 56%). The overall certainty of this evidence was rated as ‘moderate’ and downgraded for concerns regarding imprecision. Similar results were found for the maintenance of intervention effect on SBP (online supplemental figure 50).
Subgroup analysis
Stratification of exercise-only RCTs by type of exercise showed statistically significant difference in SBP (p=0.03). One study examining the impact of a Tai Chi intervention demonstrated a greater change in SBP in the exercise group compared with the control (online supplemental figure 49). The certainty of evidence was rated as ‘moderate’ (downgraded for concerns regarding imprecision). The other tests for subgroup differences were either not significantly different (timing of the intervention, p=0.26, online supplemental figure 48) or were not applicable due to insufficient data for stratifying (mode of delivery, maintenance of intervention effect)
Diastolic blood pressure
From preintervention to postintervention, the pooled summary estimate showed a greater change in DBP (mm Hg) for exercise groups as compared with the no exercise controls (9 RCTs, n=2575; MD −1.38, 95% CI −2.60 to –0.15, I2 66%; online supplemental figure 55). The overall certainty of this evidence was rated as ‘low’ and downgraded for concerns regarding inconsistency and indirectness.
The pooled summary estimate showed no difference in DBP during the maintenance phase for exercise groups as compared with the no exercise controls (4 RCTs, n=645; p=0.17; online supplemental figure 58). The overall certainty of this evidence was rated as ‘very low’ and downgraded for concerns regarding inconsistency, indirectness and imprecision.
Sensitivity analysis
The pooled summary estimate for the exercise+co-interventions was not significantly different from the pooled estimate for the exercise-only interventions (p=0.70; online supplemental figure 55). The overall certainty of this evidence was rated as ‘very low’ for exercise+co-interventions (downgraded for concerns regarding inconsistency, indirectness and imprecision) and as ‘low’ for the exercise-only interventions (downgraded for concerns regarding imprecision). Similar results were found for the maintenance of intervention effect on DBP (online supplemental figure 58).
Subgroup analysis
Stratification of exercise-only RCTs by subgroups were not significant (timing of the intervention, p=0.88, online supplemental figure 56; type of exercise, p=0.96, online supplemental figure 57) or could not be examined due to insufficient data for stratifying (mode of delivery, maintenance of intervention effect).
Other outcomes and study designs
Other outcomes and study designs are reported in the online supplement. Infant growth and development, breast milk volume and quality, and risk of injury (figure 4) were not different between exercise and control groups. Some metrics of lipid metabolism were improved with exercise (eg, very low density lipoproteins VLDL-c; triglycerides) (figure 5) but other blood markers of glucose and lipid metabolism were not.

Effects of postpartum exercise compared with control on incidence of injury (randomised controlled trials). Analyses were conducted using a random-effects model. df, degrees of freedom; M-H, Mantel-Haenszel method.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of postpartum exercise compared with control on change in triglycerides (mmol/L; randomised controlled trials). Sensitivity analyses were conducted with studies including exercise+co-interventions and exercise-only interventions. Analyses were conducted using a random-effects model. df, degrees of freedom; IV, inverse variance; PP, postpartum.
Discussion
The current systematic review and meta-analysis demonstrate that exercise during the postpartum period decreased the risk of developing type 2 diabetes and lowered cardiometabolic risk factors including triglycerides, VLDL-c and SBP. By initiating exercise in the first 12 weeks following childbirth, the risk of developing type 2 diabetes was reduced by 28%. Importantly, these improvements were observed without an adverse effect on breast milk quality or quantity, infant growth or increased odds of injury. These findings underscore the pivotal role of early postpartum exercise as a preventative means to enhance maternal cardiometabolic health.
The postpartum period exists in stark opposition to the antepartum period. In the postpartum period, maternal priorities quickly switch from their personal health and well-being to that of their newborn. Physical activity was perceived to have a potential negative impact on breastfeeding by new mothers in the postpartum period.84 However, a review on this topic published in 2002 indicated that physical activity does not influence breast milk volume or macronutrient composition or infant body weight or growth.85 A small percentage of breastfeeding individuals may perceive a decrease in infant willingness to breastfeed after maximal or submaximal maternal exercise, perhaps due to an increase in lactate in breast milk.85 The fullness of breasts prior to exercise and intensity of exercise can influence the time to peak lactate concentration and the time to postexercise decreases in lactate concentration in breast milk.86–88 However, lactate concentration in breast milk can return to values comparable to resting concentrations within 30 min of maximal intensity exercise.86 These factors may be taken into consideration when considering feeding and exercise schedules. Our review, which includes studies from the last two decades, also indicate that breast milk quality and quantity are not adversely impacted by chronic exercise. In addition, no adverse effect on infant growth was observed when mothers engaged in an exercise intervention, although the evidence was limited. Previous work has demonstrated that breastfeeding individuals have more favourable cardiometabolic profiles which may reduce long-term cardiovascular risk.7 89 90 While the decision to breastfeed is highly personal and can be influenced by a myriad of social, cultural and personal factors, these data demonstrate the compatibility of breastfeeding and exercise in the postpartum period.
There is extensive literature suggesting the preventive and therapeutic power of exercise for a wide array of medical conditions, including type 2 diabetes and cardiovascular disease. In non-postpartum populations, exercise has been found to be as effective as antihypertensive medication in reducing blood pressure.91 The present review found that exercise-only interventions were effective in decreasing SBP. The mechanisms underlying this risk reduction is multifactorial and likely dependent on the type, duration and intensity of exercise. Aerobic and resistance exercise have been demonstrated to improve vascular health (improved endothelial function, decreased arterial stiffness), glucose uptake and transport, and insulin sensitivity, and reduce inflammation, among others.92–94
In the current review, we identified that exercise+co-interventions decreased the odds of developing type 2 diabetes by 28%. Additionally, initiating an exercise intervention in the first 12 weeks following childbirth was associated with greater decrease in the odds of diabetes and low density lipoproteins compared with later in the postpartum period. Furthermore, exercise-only and exercise+co-interventions demonstrated a decrease in triglycerides during the postpartum period. These data emphasise the importance of a gradual return to activity that balances the required healing and recovery from pregnancy and childbirth, with the opportunity to improve cardiometabolic health. Additional research further investigating the optimal intensity, duration or type of exercise to prevent or delay the development of cardiovascular disease or diabetes is essential.
During the postpartum period, the majority of physiological adaptations to pregnancy revert back to the non-pregnant state.95 However, the transient changes of pregnancy including the alterations to hormonal balance, posture and bone metabolism may have a persisting effect on risk of injury. Postpartum injuries range in severity, from mild to severe, and the most common areas affected include the pelvis,11 perineum,12 abdominal13 and back regions,11 including damage to soft, hard and neural tissues. The risk of postpartum injury is influenced by a multitude of factors affecting all those in the postpartum period. These factors include: mode of delivery (vaginal vs caesarean section), young (<19 years old) or advanced (>35 years old) maternal age, obesity/high body mass index (>25 kg/m2), prolonged labour, and instrument-assisted delivery including the use of forceps or vacuum devices.14 15 The underlying mechanisms responsible for the development of injuries postpartum resulting in a higher prevalence of injuries in active postpartum individuals is not well understood.96 There is very limited evidence on injury and physical activity during the postpartum period. The findings of this review demonstrated that based on limited currently available evidence there is no increased odds of injury in the postpartum period.
Strengths of this review include our broad inclusion criteria considering all publication designs (except case studies and secondary studies), dates and languages. We applied rigorous methodology (PRISMA, JBI, GRADE) to guide the systematic review process and quality of evidence assessment.18 30 97 Change scores, subgroup analyses (exercise-only vs exercise+cointerventions) and stratified analyses allowed detailed consideration of both heterogeneity and the influence of various factors (time postpartum, mode of exercise delivery, type of activity) on review outcomes; however, statistical heterogeneity was still moderate within certain subgroups. Essential next steps include further research to determine optimal type, duration and intensity of postpartum exercise.
Limitations of the current review included a lack of standardised definition of postpartum injury. One major limitation of this study was a lack of ‘high’ quality evidence from RCTs to build the body of evidence. A majority of the RCTs were downgraded from ‘high’ to ‘low’ evidence because of imprecision, due to small sample size, that is, lack of power to detect differences with precision, and indirectness (ie, exercise intervention was combined with other interventions, such as nutrition). Another limitation was a lack of research on exercise during the postpartum period that focuses on the outcomes of interest in the current paper. Although there is no definition of postpartum injury used clinically or in research, a definition of injury is critical for consistency as well as interpretation and implementation of research studies.
Further research is certainly required in all of these domains, particularly on the relationship between postpartum exercise and injury. It is vital to standardise the definition of postpartum injury and increase reporting of instances of injury during this time. Additionally, further subgroup analysis regarding the type and timing of intervention will be paramount in understanding potential interactions between injury, mode of delivery and delivery/postpartum complications. Furthermore, there is a lack of literature regarding postpartum exercise and infant growth and development. While this review begins to demonstrate that there are no adverse effects of postpartum exercise on breast milk quality or quantity, there is a lack of data investigating the composition of breast milk. All of these factors directly influence infant growth and development.
Conclusion
Postpartum exercise is emerging as a promising strategy to reduce the risk of hypertension and diabetes during the postpartum period without increased risk of harm to breast milk supply or quality, infant growth, or maternal injury.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @ExercisePreg
Correction notice This article has been corrected since it published Online First. The guideline title has been amended to: Canadian Society for Exercise Physiology 2025 Canadian Guideline for Physical Activity, Sedentary Behaviour and Sleep throughout the First Year Postpartum.
Contributors MHD, S-MR, MUA, KF contributed to the conception of the study. MHD, S-MR, MUA, AS contributed to the design of the study and development of the search strategy. AS conducted the systematic search. PATJ, AM, TS, SM, JBW completed the acquisition of data. AM, PATJ performed the data analysis. MHD, S-MR, MUA, PATJ, AM assisted with the interpretation. PATJ and MHD were the principal writers of the manuscript. All authors contributed to the drafting and revision of the final article. All authors approved the final submitted version of the manuscript. MHD is the guarantor.
Funding AM is funded by a Mitacs Studentship. MHD is funded by a Christenson Professorship in Active Healthy Living. S-MR is funded by the Université du Québec à Trois-Rivières research chair in physical activity and maternal and neonatal health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.