Article Text

Abstract
Objective To evaluate systematic reviews of randomised controlled trials (RCTs) on the effects of exercise on general cognition, memory and executive function across all populations and ages.
Methods Systematic reviews and meta-analyses of RCTs evaluating the effects of exercise on general cognition, memory and executive function were eligible. Data extraction and risk of bias scoring were conducted in duplicate. The A MeaSurement Tool to Assess systematic Reviews (AMSTAR-2) was used to assess the risk of bias. Effect sizes were pooled using random effects models and reported as standardised mean differences (SMD). Subgroup analyses were conducted for participant and intervention characteristics.
General cognition, memory and executive function.
Data sources CINAHL, The Cochrane Library, Embase, MEDLINE via OVID, Emcare, ProQuest Central, ProQuest Nursing and Allied Health Source, PsycINFO, Scopus, Sport Discus and Web of Science.
Results 133 systematic reviews (2,724 RCTs and 258 279 participants) were included. Exercise significantly improved general cognition (SMD=0.42), memory (SMD=0.26) and executive function (SMD=0.24). Memory and executive function improvements from exercise were greater for children and adolescents than for adults and older adults. Those with attention-deficit/hyperactivity disorder exhibited greater improvement in executive function than other populations. Effects were generally larger for low- and moderate-intensity interventions. Shorter interventions (1–3 months) and exergames (video games that require physical movement) had the largest effects on general cognition and memory. Findings remained statistically significant after excluding reviews rated as low and critically low quality.
Conclusions These findings provide strong evidence that exercise, even light intensity, benefits general cognition, memory and executive function across all populations, reinforcing exercise as an essential, inclusive recommendation for optimising cognitive health.
Trial registration number PROSPERO ID: CRD42023468991.
- Exercises
- Aging
- Psychiatry
- Risk factor
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article and its supplementary information files.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Cognitive decline and related neurodegenerative diseases are global health concerns.
Effective strategies to preserve and enhance cognitive function across the lifespan are urgently required.
WHAT THIS STUDY ADDS
Exercise interventions significantly improved general cognition, memory and executive function across all populations and ages.
Those with attention-deficit/hyperactivity disorder exhibited greater improvement in executive function from exercise interventions than the general population and other clinical groups.
Effects were generally larger for low- and moderate-intensity interventions.
These results offer compelling evidence that exercise, even at a lighter intensity, positively impacts overall cognitive function, memory and executive skills in all demographic groups.
Introduction
In recent decades, an increasing body of research has evaluated the relationship between exercise and cognitive function.1 2 Cognitive function encompasses a broad spectrum of mental processes, including memory, attention and executive functions, all of which play pivotal roles in an individual’s daily life and overall well-being.3 4 Cognitive decline and related neurodegenerative diseases have become global health concerns, underscoring the urgency of identifying effective strategies to preserve and enhance cognitive function across the lifespan.5
Exercise has profound effects on physical health.6 7 However, increasing evidence suggests that these effects extend beyond physical health, positively influencing cognitive health8 and mental well-being.9 The relationship between exercise and cognitive function has become an important area of research due to its relevance to healthcare and the broader community. Given the growing interest in the topic area, many systematic reviews have emerged in recent years, each with its own unique scope and methodology. While each of these reviews has provided valuable insight into the impact that exercise can have on cognitive function and memory, they are often limited to specific populations (ie, older adults or children),10 11 particular conditions (ie, Alzheimer’s disease12 or attention deficit disorder13 and specific forms of exercise (ie, resistance exercise14 or yoga).15 There is a need to comprehensively evaluate the impact of all exercises on general cognition, memory and executive function across all populations.
To the authors’ knowledge, only one systematic review of systematic reviews (ie, an umbrella review) has examined the effect of exercise on cognition.16 Results indicate that exercise had a small positive effect on cognition (d=0.22, 95% CI 0.16 to 0.28), although this effect became negligible after correcting for publication bias (d=0.05, 95% CI −0.09 to 0.14).16 This umbrella review by Ciria et al 16 provided valuable insights into the effects of aerobic and resistance exercise on cognition in healthy populations, employing innovative statistical techniques to address publication bias and focusing on primary randomised controlled trials (RCT) data. In a subsequent letter to the editor, Ciria et al 17 performed additional analyses that extended their original work, examining moderators such as participant characteristics (eg, age, sex and baseline activity levels), intervention characteristics (eg, intensity, type and duration) and cognitive domains. These analyses reinforced their conclusion that the effects of exercise on cognition are inconclusive, even when accounting for these moderators. Their findings, while valuable, remain limited in scope, as the review exclusively focused on healthy populations and excluded individuals who might derive the greatest benefit from exercise interventions, such as those with cognitive impairment or chronic diseases. Moreover, the analyses did not encompass mind-body exercises like yoga or Tai Chi, which may confer unique cognitive benefits. These limitations underscore the need for a larger, more comprehensive synthesis of systematic reviews to evaluate the effects of various exercise modalities across both clinical and non-clinical populations and all age groups. Therefore, this umbrella review seeks to systematically evaluate all existing systematic reviews and meta-analyses on the effects of exercise on general cognition, memory and executive function across all populations, including children, adolescents and adults, and clinical and non-clinical populations.
Methods
Protocol and registration
The protocol for this umbrella review was preregistered on PROSPERO (ID: CRD42023468991), and the findings are reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18
Selection criteria and search strategy
The inclusion criteria were developed using the population, intervention, comparison, outcomes and study type (PICOS) framework. Population: any human population (children, adolescents, adults, healthy and clinical); Intervention: reviews that evaluated exercise interventions were included. The following definition of exercise was used: ‘a type of physical activity consisting of planned, structured and repetitive bodily movement done to improve and/or maintain physical fitness’.6 Reviews were included if ≥75% of the included RCTs focused solely on exercise, including (but not limited to) aerobic or resistance exercise, yoga, dance, Tai Chi and exergames, which were not combined with any other intervention. Reviews evaluating regular exercise training of at least 4 weeks were included irrespective of exercise mode, supervision, delivery, intensity or weekly duration. Comparator: reviews were eligible if ≥75% of the included RCTs compared exercise to no intervention, waitlist, usual care, nothing, a sham intervention, an equal attention non-exercise intervention arm or a lower/lesser exercise intervention. Outcomes: any assessment of general cognition, memory or executive function. Study type: systematic reviews that included meta-analyses. Reviews were excluded if they included any non-RCTs or studies assessing single bouts of exercise.
Databases were searched (CINAHL, The Cochrane Library, Embase via OVID, MEDLINE via OVID, Emcare via OVID, ProQuest Central, ProQuest Nursing and Allied Health Source, PsycINFO, Scopus, Sport Discus via Ebscohost and Web of Science) using subject heading, keyword and MeSH term searches for ‘systematic review’, ‘meta-analysis’, ‘cognitive function’, ‘memory’, ‘executive function’, and ‘exercise’ (see online supplemental table 1 for the full search strategy). Database searches were limited to peer-reviewed journal articles published in English-language from inception to 1 November 2023.
Supplemental material
Data management and extraction
All search results were imported into EndNote X9 (Clarivate, Philadelphia, Pennsylvania, USA) to remove duplicates. Records were then exported to Covidence (Veritas Health Innovation, Melbourne, Australia) for title/abstract and full-text screening, data extraction and risk of bias scoring. All screening was completed in duplicate by two independent reviewers, with disagreements resolved by discussion and consultation with a third reviewer.
Data extraction and risk of bias scoring were conducted in duplicate by two independent reviewers, and discrepancies were resolved through discussion and consultation with a third reviewer. A standardised extraction form was used to extract information on study details, population characteristics, intervention characteristics, outcomes of interest and results. The A MeaSurement Tool to Assess systematic Reviews (AMSTAR-2) tool was used to assess the risk of bias of the included reviews by two independent reviewers in duplicate.19 The AMSTAR-2 consists of 16 items, each scored as ‘Yes’, ‘Partial Yes’ or ‘No’, of which seven items are considered ‘critical’ and nine are ‘non-critical’.19 The following items are considered critical: protocol registration, adequacy of search strategy, justification for excluding individual studies, risk of bias assessment, appropriateness of meta-analysis methods, use of risk of bias during interpretation and assessment of publication bias. Reviews were scored as ‘high confidence’ (no critical weakness and <3 non-critical weaknesses), ‘moderate’ (1 critical weakness and <3 non-critical weaknesses), ‘low’ (>1 critical weakness and <3 non-critical weaknesses) or ‘critically low’ (>1 critical weakness and ≥3 non-critical weaknesses).19
Umbrella review synthesis methods
The Corrected Covered Area (CCA) method was used to assess overlap in the RCTs that were included across all eligible reviews.20 A CCA score of 0% indicates that every included review consisted of entirely unique RCTs, while a score of 100% indicates that every eligible review included the same RCTs. The following cut-offs were used: 0%–5%: ‘slight overlap’; 6%–10%: ‘moderate’; 11%–15%: ‘high’ and >15%: ‘very high’ overlap.21
Meta-analyses for general cognition, memory and executive function were performed by pooling the effect sizes and 95% CIs reported in each review, using a random effects model. Meta-analyses were conducted using standardised mean differences (SMD) as the primary effect measure. Meta-analyses were also performed using mean differences (MD) if sufficient data were available. The Cattell-Horn-Carroll-Miyake Model of Cognition for Clinical Assessment22 was used to categorise the tests. Tests of working memory were categorised as executive function.23 Results of all meta-analyses were displayed visually using forest plots. Subgroup analyses were performed for age group (children/adolescents, adults and older adults (aged 65 years and older)), population (general population, ie, individuals who are otherwise healthy and not diagnosed with any cognitive impairment, chronic illnesses, or medical conditions, cognitive impairment status, clinical condition or chronic disease status), exercise mode (aerobic, resistance, mixed mode, mind-body (yoga and Tai Chi)), dance, exergames, other (which consisted of a variety of sports and martial arts)), exercise intensity (low, moderate, moderate-to-vigorous and vigorous, based on the intensity reported in the systematic reviews), intervention length (1–3 months, 4–6 months and >6 months), session frequency (1–2/week, 3–5/week and 6–7/week), session duration (<30 min, 30–60 min and >60 min), weekly duration (<150 min/week and ≥150 min/week) and risk of bias score (critically low, low, moderate and high confidence). We defined a systematic review and meta-analysis as focusing on ‘adults’ if more than 75% of the included RCTs recruited participants aged 18–65 years, regardless of cognitive status. The I2 statistic was used to quantify the proportion of the overall outcome attributed to variability.24 The following values were used: 0%–29%: no heterogeneity; 30%–49%: moderate heterogeneity; 50%–74%: substantial heterogeneity and 75%–100%: considerable heterogeneity.25 The following classifications for the magnitude of effect for SMD were used: <0.20: small effect; 0.20–0.50: medium effect and >0.50: large effect.26 A p value of <0.05 was considered statistically significant. Funnel plots were created to investigate publication bias by assessing for the presence of asymmetries.27 Additionally, trim-and-fill analyses were conducted on meta-analyses containing at least 10 studies to account for potential unpublished studies.27 The trim-and-fill analyses were not prespecified in the registered protocol but were conducted post hoc to address potential publication bias. All meta-analyses were performed using Stata/MP (V.16, Stata Corp, College Station, Texas, USA).
The Oxford Centre for Evidence-based Medicine levels of evidence and grades for recommendations28 were used to classify the overall level of evidence as follows: A: consistent Level 1 studies (systematic reviews of RCTs); B: consistent Level 2 (systematic reviews of cohort studies) or Level 3 studies (systematic reviews of case-control studies) or extrapolations from Level 1 studies; C: Level 4 studies (case series) or extrapolations from Level 2 or Level 3 studies or D: Level 5 evidence (expert opinion without critical appraisal) or inconclusive evidence.28
Equity, diversity and inclusion statement
The author team is comprised of student and senior researchers across various disciplines. A wide range of demographic, socioeconomic and cultural backgrounds were included in the study populations, including from low- and middle-income countries.
Patient and public involvement
There was no patient or public involvement in this umbrella review.
Results
A total of 6620 results were identified following a database search, of which 133 reviews were included. The PRISMA flowchart, including reasons for exclusions, is shown in figure 1. A full list of reasons for full-text exclusions is shown in online supplemental table 2. The 133 included reviews comprised 2724 unique (component) RCTs and a total of 258 279 participants. The overall CCA was 0.78%, indicating a slight overlap.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. RCTs, randomised controlled trials.
An overview of age groups, populations and exercise intervention characteristics is shown in online supplemental table 3. Over half (n=77) of the included reviews were from China (affiliation of the first author). Mean participant age ranged between 6.8 and 89.2 years, and most reviews (n=130) included both female and male participants. 72 reviews focused on older adults, 47 focused on adults, 11 on children and 3 involved children and adults. Most reviews evaluated mixed-mode exercise (n=103), while 30 evaluated single types of exercise. These included aerobic (n=7), resistance (n=5), Tai Chi (n=5), dance (n=5), exergames (n=4), yoga (n=2) and Baduanjin (n=2). Most reviews (n=94) had a critically low AMSTAR-2 score (low: n=19 and high: n=20, online supplemental table 4). Common limitations included not providing a list of full-text exclusions (n=123) and not describing the funding sources (n=116).
Meta-analysis results
General cognition
Pooled analysis of 107 meta-analyses (n=82 742 participants) showed a significant effect of exercise for improving general cognition (SMD=0.42, 95% CI 0.37 to 0.47, I2=82.73%, p<0.01, online supplemental figure 1). There were sufficient MD data for the following instruments: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MOCA) and the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog; online supplemental table 5). Effect sizes for each instrument were: MMSE=1.54 (95% CI 1.11 to 1.98), MOCA=2.31 (95% CI 1.98 to 2.64), ADAS-Cog=−1.48 (95% CI −2.54 to 0.41; note negative values for ADAS-cog represent an improvement; test of subgroup differences: Qb(2)=47.10, p<0.01).
Grade of recommendation: (A) Consistent level 1 studies.
Memory
Pooled results from 62 meta-analyses (n=50 975 participants) showed a significant effect of exercise for improving memory (SMD=0.26, 95% CI 0.20 to 0.32, I2=78.16%, p<0.01, online supplemental figure 2). Most of the tests included in this domain are traditionally referred to as short-term memory or episodic memory. There were sufficient MD data for the Wechsler Memory Scale and the Verbal Learning Test (online supplemental table 5). MD effect sizes were: Wechsler Memory Scale=10.71 (95% CI 4.22 to 17.21) and the Verbal Learning Test: 1.08 (95% CI 0.73 to 1.43) (test of subgroup differences: Qb(4)=28.46, p<0.01).
Grade of recommendation: (A) Consistent level 1 studies.
Executive function
Pooled results from 117 meta-analyses (n=107, 242 participants) showed a significant effect of exercise for improving executive function (SMD=0.24, 95% CI 0.21 to 0.27, I2=70.34%, p<0.01, online supplemental figure 3). There were sufficient MD data for the following instruments: Digit Span Test, Digit Span-Backward, Digit Span-Forward, Trail Making Test Part A and B (TMT-A and TMT-B; see online supplemental table 5). MD effects were: Digit Span Test: 0.92 (95% CI 0.29 to 1.55); Digit Span-Backward: 0.15 (95% CI −0.14 to 0.43); Digit Span-Forward=0.40 (95% CI 0.22 to 0.58); TMT-A=−2.03 (95% CI −5.47 to 1.41) and TMT-B=−8.68 (95% CI −15.48 to –1.88; note negative values for TMT-A and B represent an improvement; test of subgroup differences: Qb(1)=2.92, p=0.09, online supplemental table 5).
Grade of recommendation: (A) Consistent level 1 studies.
Subgroup analyses
Results of subgroup analyses for age and population are shown in figure 2 (general cognition), figure 3 (memory) and figure 4 (executive function). Results of subgroup analyses for exercise mode, intensity, intervention length, session frequency, session duration and weekly duration are shown in online supplemental table 6 (general cognition), 7 (memory) and 8 (executive function).

Subgroup analyses for age and population for general cognition. REML, restricted maximum likelihood.

Subgroup analyses for age and population for memory. REML, restricted maximum likelihood.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
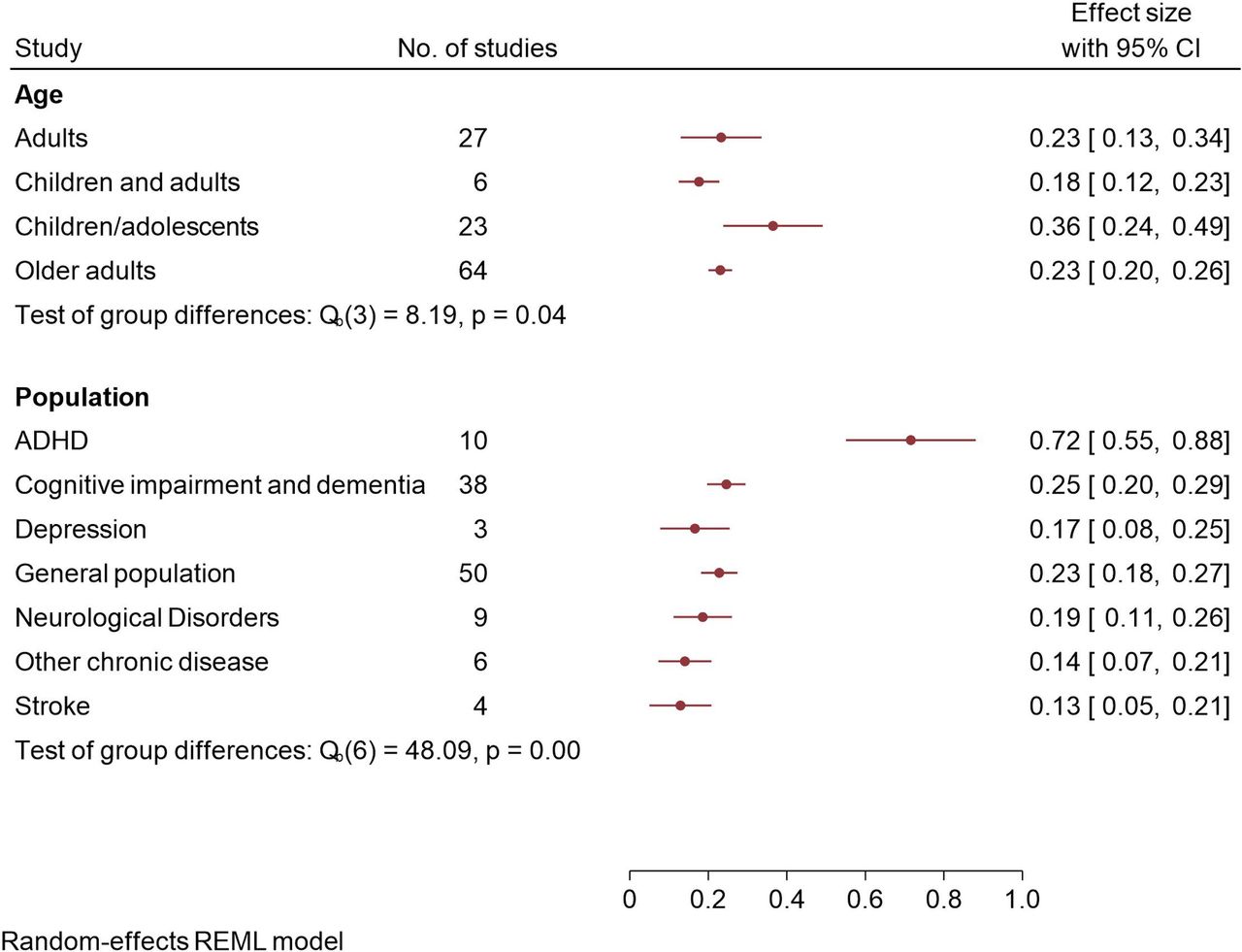
Subgroup analyses for age and population for executive function. REML, restricted maximum likelihood.
Age group and population
General cognition
Exercise was associated with improvements in general cognition across all age groups, with no significant differences observed between studies involving adults, children and older adults (SMD range=0.28–0.42; test of group differences: Qb(2)=4.09, p=0.13, figure 2). Similarly, cognitive benefits were consistent across various clinical populations, with no significant differences between groups (SMD range=0.28–0.47; test of group differences: Qb(5)=3.93, p=0.56, figure 2).
Memory
Differences were observed for age, with children/adolescents showing larger improvements in memory (SMD=0.85) compared with studies involving adults and older populations (SMD range=0.18–0.27; test of group differences: Qb(3)=19.16, p<0.01, figure 3). Memory benefits were consistent across various clinical populations, with no significant differences between groups (SMD range=0.13 to 0.38; test of group differences: Qb(4)=9.62, p=0.05, figure 3).
Executive function
Exercise was associated with improvements in executive function across all age groups, with the largest benefits observed in children/adolescents (SMD=0.36) compared with other ages (SMD range=0.18–0.23; test of group differences: Qb(3)=8.19, p=0.04, figure 4). Tests of subgroup differences showed that exercise interventions were most effective for improving executive function in attention-deficit/hyperactivity disorder (ADHD; SMD=0.72) compared with cognitive impairment and dementia, depression, the general population, neurological disorders, other chronic disease and stroke (SMD range=0.13–0.25; test of group differences: Qb(6)=48.09, p<0.01, figure 4).
Exercise mode
General cognition
Significant subgroup effects were observed for exercise mode, with moderate-to-large effects observed for exergames on general cognition (SMD=0.61), while small-to-moderate effects were observed for aerobic, dance, mind-body, mixed mode, resistance exercise and other (SMD range=0.25–0.44; test of subgroup differences: Qb(6)=19.38, p<0.01, online supplemental table 6).
Memory
Exercise mode also had significant effects on memory, with large effects observed for exergames (SMD=0.58) and small-to-medium effects observed for aerobic, dance, mind-body, mixed mode and resistance exercise (SMD range=0.13–0.51; test of subgroup differences: Qb(5)=28.02, p<0.05, online supplemental table 7).
Executive function
The positive effects of exercise on executive function differed based on exercise mode, with other forms of exercise (SMD=0.45) having a greater effect compared with aerobic, dance, exergames, mind-body, mixed mode and resistance exercise (SMD range=0.12–0.37; test of subgroup differences: Qb(6)=13.29, p=0.04, online supplemental table 8).
Exercise intensity
General cognition, memory and executive function
The beneficial effect of exercise on general cognition (test of subgroup differences: Qb(3)=2.61, p=0.46, online supplemental table 6), memory (test of subgroup differences: Qb(2)=1.40, p=0.50, online supplemental table 7) or executive function (test of subgroup differences: Qb(3)=3.69, p=0.30, online supplemental table 8) did not differ based on exercise intensity.
Intervention length
General cognition, memory and executive function
Interventions that were 1–3 months had the greatest effect on general cognition (SMD=0.39), compared with 4–6 month and >6 month interventions (SMD range=0.20–0.30; Qb(2)=7.53, p=0.02, online supplemental table 6). The beneficial effect of exercise on memory and executive function was consistent across different intervention durations, with no significant differences observed for memory (Qb(2)=2.12, p=0.35, online supplemental table 7) or executive function (test of subgroup differences: Qb(2)=0.67, p=0.72, online supplemental table 8).
Session frequency
General cognition, memory and executive function
The beneficial effects of exercise across cognitive domains did not significantly differ based on session frequency for general cognition (test of subgroup differences: Qb(2)=6.02, p=0.05, online supplemental table 6), memory (test of subgroup differences: Qb(2)=0.76, p=0.68, online supplemental table 7) and executive function (test of subgroup differences: Qb(2)=0.95, p=0.62, online supplemental table 8).
Session duration
Cognition, memory and executive function
The beneficial effect of exercise across cognitive domains did not significantly differ based on session duration (general cognition: test of subgroup differences: Qb(2)=5.68, p=0.06, online supplemental table 6; memory: test of subgroup differences: Qb(2)=1.91, p=0.75, online supplemental table 7; executive function: test of subgroup differences: Qb(2)=0.81, p=0.67, online supplemental table 8).
Weekly duration
General cognition, memory and executive function
The beneficial effect of exercise across cognitive domains did not differ based on weekly exercise duration for general cognition (test of subgroup differences: Qb(1)=0.10, p=0.75, online supplemental table 6) or executive function (test of subgroup differences: Qb(1)=2.88, p=0.09, online supplemental table 8). There was an insufficient number of studies to assess differences in memory.
Risk of bias score
General cognition, memory and executive function
Subgroup analyses for the risk of bias score are shown in online supplemental table 9. There was a consistent pattern for the benefits of exercise to be larger in critically low-confidence studies relative to low- and high-confidence studies. For instance, the impact of exercise on general cognition, the SMD based on critically low studies, was 0.43 versus 0.23–0.38 for low- and high-confidence studies (test of subgroup differences: Qb(2)=25.26, p<0.01). For memory, the SMD from critically low-confidence studies was 0.30 versus 0.13–0.22 for low- and high-confidence studies (test of subgroup differences: Qb(2)=9.46, p=0.01). For executive function, the SMD from critically low studies was 0.26 versus 0.16–0.19 for low- and high-confidence studies (test of subgroup differences: Qb(2)=7.32, p=0.03).
Sensitivity analyses and publication bias
We conducted unplanned sensitivity analyses by excluding the study by Stanmore et al 29 due to identified methodological issues and inaccurate effect size.30 After excluding this study, the effect size for general cognition changed from 0.61 to 0.70 and executive function changed from 0.37 to 0.26. Visual inspection of the funnel plots for general cognition, memory and executive function (online supplemental figure 4) each displayed a degree of asymmetry with a gap in the bottom left quadrants, suggesting a lack of smaller studies reporting negative effect sizes. The estimated true effect sizes, or theta (θ), for general cognition, memory and executive function were d=0.31, d=0.24 and d=0.20, respectively.
Discussion
This is the first study examining the effects of various exercise modalities on general cognition, memory and executive function across all populations. It included 133 systematic reviews and meta-analyses comprising over 2700 RCTs and over 250 000 participants. Overall, exercise interventions improved general cognition, memory and executive function with a small-to-moderate effect across the lifespan and health status. Children/adolescents and those with ADHD experienced the greatest improvements in memory and executive function, respectively. All exercise modalities were effective, with exergames benefiting cognition most and mind-body exercises benefiting memory most. Gains were unaffected by frequency, duration or intensity, but 1–3 month interventions showed larger cognitive improvements than longer ones. Higher study quality suggested more modest yet significant cognitive benefits than lower-quality studies.
Our umbrella review provides compelling evidence that exercise provides benefits across general cognition, memory and executive function. Importantly, these significant benefits hold even when critically low- and low-quality studies are excluded from estimates and when publication bias is considered. For example, in our study, the SMD for general cognition was small to medium (d=0.42), remaining small to medium after accounting for publication bias (d=0.30) and reducing to small (d=0.23) when only high-quality studies were meta-analysed. This contrasts with the findings of Ciria et al,16 which reported smaller overall effects (d=0.22) that became negligible after accounting for publication bias (d=0.05).
The differences in estimates between the two studies may be attributed to their different samples: Ciria et al’s review was limited to healthy participants and included 24 meta-analyses encompassing a total of 109 primary studies involving 11 206 participants. In contrast, our umbrella review included fivefold more meta-analyses (133 systematic reviews), encompassing 25-fold more primary studies (2724 RCTs) and 23-fold more participants (n=258 279). Furthermore, our meta-analyses of MD showed significant improvement in general cognition based on MMSE and MOCA; however, these tests generally focused on adults. Tests conducted with children included the Wechsler Intelligence Scale for Children, the Kaufman Assessment Battery for Children, the Stroop Colour-Word Test, the Digit Span Test, the Wisconsin Sorting Test and the Verbal Learning Test. However, there was insufficient data to perform meta-analyses using MD. It is important to note that many of the cognitive assessment tools used in these studies, particularly the MMSE, MoCA and ADAS-Cog, are primarily designed to detect cognitive impairment rather than differentiate between levels of cognitive function in healthy middle-aged adults. As such, these measures likely exhibit ceiling effects in cognitively intact populations, potentially limiting their sensitivity to exercise-induced changes in this demographic. Given the comprehensive nature and scale of this umbrella review, which includes a vast number of studies and participants across diverse populations and exercise modalities, our findings underscore the robust nature of exercise as a modifier of cognitive function.
The mechanisms underpinning the cognitive benefits of exercise are likely physiological and psychological. Physiologically, exercise may bolster cognition through mechanisms such as the augmented release of neurotrophic factors,8 increased vascularisation of the brain,31 greater dendritic spine density,32 enhanced synaptic plasticity33 and reduced systemic inflammation.34 Psychologically, the social and interactive aspects of exercise may further catalyse cognitive improvements.35 While our analysis revealed that all exercise modalities confer significant improvements in general cognition, memory and executive function, certain modalities impart greater cognitive benefits. Our findings highlight the cognitive potency of exergaming, which likely merges physical exertion with cognitively stimulating tasks, enhancing general cognition through the dual demands of physically and mentally demanding tasks that require participants to recall movements, recognise visual and verbal cues and memorise sequences and steps.36 Similarly, the practice of mind-body exercises (including yoga, Tai Chi and Baduanjin), which requires a high degree of attention in conjunction with the memorisation of coordinated movement sequences,37 was found to be particularly beneficial for memory enhancement. While our findings indicate that low-intensity exercise had the greatest effect on cognitive outcomes, it is important to consider that many low-intensity interventions, such as Tai Chi, yoga and exergaming, incorporate significant cognitive components.36 38 These activities often involve complex movement patterns, mindfulness practices and mental engagement that may contribute to cognitive stimulation independently of physical exertion. For instance, Tai Chi requires memorisation of sequences and spatial awareness, yoga emphasises mind-body connection and breath control, and exergaming typically involves problem-solving and quick decision-making. Therefore, the consistent effectiveness of cognitively engaging low-intensity exercises across various cognitive outcomes raises the question of whether the benefits are primarily due to the physical intensity or the cognitive engagement inherent in these activities.39 Several mechanisms may contribute to the cognitive benefits observed in low-intensity exercise interventions. These include increased cerebral blood flow, enhanced neuroplasticity, improved neurotransmitter function and the cognitive demands of complex movement patterns.39 40 Future research should aim to disentangle the effects of exercise intensity from the cognitive engagement inherent in these activities to better understand the mechanisms driving cognitive improvements. This could involve comparing low-intensity exercises with varying levels of cognitive demand or isolating the physical and cognitive components of these interventions. Additionally, longitudinal studies examining the long-term cognitive effects of different types of low-intensity exercise could provide valuable insights into the relative contributions of physical intensity versus cognitive engagement in promoting cognitive health.
Interestingly, our analysis indicates that interventions of shorter duration (≤3 months) were more efficacious than those extending beyond 6 months for general cognition and memory. Although this finding may seem counterintuitive, similar findings were reported in an umbrella review of the effects of exercise on depression and anxiety.9 One plausible explanation for this is the higher attrition and lower adherence rates commonly associated with lengthier interventions.41 Alternatively, a lack of exercise progression over the long term may be a factor contributing to the diminishing benefits of an exercise regimen. Similarly, it is possible that the novelty of an exercise regimen, which diminishes with time, may be crucial for eliciting cognitive improvements. As participants adapt to the regimen, its cognitive and physiological challenges—and hence its benefits—may wane due to the lack of progression or increased difficulty in the exercise routine. Neuroimaging studies have demonstrated that even short-term interventions of 1–3 months can elicit significant changes in brain structure and function, including alterations in grey matter volume, functional connectivity and activation patterns in regions associated with cognitive functions.42–45 How these structural and functional brain changes related to behavioural outcomes require further appropriately powered studies. Notably, the beneficial cognitive outcomes of exercise documented in this study were independent of session frequency, duration or intensity. This corroborates existing evidence that negates a dose-response relationship between exercise volume and cognitive enhancements, underscoring the potential for even minimal, low-intensity exercise to confer cognitive benefits.46 47 This insight is significant as it promotes the inclusivity and feasibility of a range of exercise interventions across diverse populations and settings. The finding that exercise interventions of 1–3 months duration appear to be most efficacious may also be influenced by potential learning effects, as well as the type of comparator group used in these studies. Many shorter-term RCTs tend to use “do-nothing” or waitlist control groups, which, while minimising dropout rates, may also introduce biases that affect the interpretation of the results. Furthermore, it is important to note that shorter-term studies, particularly those with durations of 1–3 months, often have a higher risk of bias due to the use of less rigorous control groups and the potential for learning effects. These factors must be considered when interpreting the positive findings observed in these studies, as longer-term trials with more robust control conditions are needed to confirm the long-term efficacy of exercise interventions. While our findings indicate that low-intensity exercise had the greatest effect on cognitive outcomes, this result requires careful interpretation. Many low-intensity interventions, such as tai chi, yoga and exergaming, incorporate significant cognitive components that may contribute to cognitive stimulation independently of physical exertion. The effect may be most pronounced in sedentary individuals, for whom even small increases in physical activity can lead to significant cognitive gains. However, it remains unclear whether the benefits are primarily due to the physical intensity or the cognitive engagement inherent in these activities. The cognitive benefits for those who are already active may be more limited. Future research should aim to disentangle the effects of exercise intensity from cognitive engagement, clarify the differential effects across various baseline activity levels and explore the specific neurobiological mechanisms underlying these cognitive improvements. This approach will help us better understand the relative contributions of physical intensity versus cognitive engagement in promoting cognitive health.
While three studies in our analysis reported brain changes following exercise interventions, it is crucial to examine the specific characteristics of these studies. These studies focused on specific populations, such as children and adolescents, whose neuroplasticity differs from that of older adults, which may explain the observed effects in these studies. One of the three studies that reported brain changes did not include between-group comparisons but rather assessed within-group changes, which limits the generalisability of the findings. The absence of a direct comparison between the exercise and control groups reduces the ability to draw conclusions about the relative efficacy of the intervention. The majority of the included studies were rated as critically low in quality, which limits the strength of the conclusions that can be drawn from this analysis based on our synthesis of the systematic reviews. However, it is important to note that our assessment focused on the quality of the systematic reviews themselves, not the RCTs within each review. Therefore, this does not imply that the RCTs were of low quality. When focusing on high-confidence studies only (based on the risk of bias score), the effect sizes were 0.23 (95% CI 0.17 to 0.29) for general cognition, 0.22 (95% CI 0.12 to 0.32) for memory and 0.16 (95% CI 0.10 to 0.23) for executive function. Emphasising high-quality evidence ensures that clinical recommendations and interventions are grounded in robust research, enhancing the potential for meaningful improvements in cognitive outcomes.
While exercise was seen to have a moderate and similar positive impact across all populations with respect to general cognition and memory, benefits for executive function were particularly marked in individuals with ADHD. This subgroup was unique in demonstrating a large effect size. This could be attributed to the task selection and the fact that many ADHD studies involved children. While the exact reason for this finding is unclear, there is evidence to suggest that impairments in executive function are common among individuals with ADHD.48 As such, it is plausible that this population may have a greater capacity for improvement due to starting from a lower baseline, compared with those with ‘normal’ executive function. Memory tests in studies involving children with ADHD primarily included validated working memory tasks such as digit span and n-back tasks. Proposed mechanisms for working memory deficits in ADHD include altered neural activity in frontoparietal systems and reduced working memory task-specific brain activation.49 50 Exercise may improve these deficits through enhanced cerebral blood flow and neuroplasticity, though more research is needed to confirm this in ADHD populations. ADHD-specific factors, such as differences in neural processing efficiency and potential dopamine dysregulation, may contribute to working memory deficits.50 51 Exercise interventions could potentially address these factors, suggesting distinct benefits for ADHD populations. Additionally, exercise may indirectly improve cognitive function by enhancing behavioural factors often impaired in ADHD, such as attention, impulse control and hyperactivity. These improvements could lead to better task engagement and performance on cognitive tests.
Future research should aim to differentiate the direct neurobiological effects of exercise from its indirect behavioural benefits in ADHD, potentially through comparative longitudinal studies with non-ADHD populations. This approach could help clarify whether improvements in working memory result from physical activity, cognitive engagement or changes in ADHD-specific behavioural symptoms. Additionally, studies should examine whether cognitive benefits are mediated by improvements in attention, impulse control and hyperactivity, or if they occur independently of these changes. Furthermore, exploring how factors such as age, control group type, adherence and attrition moderate the effectiveness of exercise interventions will be crucial for understanding the variability in outcomes across different populations and intervention durations. There is also a need for well-designed studies examining the effects of exercise on cognition in healthy middle-aged adults using assessment tools sensitive enough to detect subtle differences in cognitive performance. Such studies should employ cognitive measures specifically validated for use in healthy populations, such as computerised cognitive batteries or more challenging executive function tasks, rather than relying solely on screening tools designed to detect cognitive impairment.
Clinical implications
This comprehensive umbrella review highlights several key implications for future research and clinical practice. For future studies, there is a critical need for more high-quality systematic reviews and meta-analyses, given the predominantly low methodological quality of included reviews. Additionally, further research should explore optimal exercise modalities, intensities, frequencies and durations tailored to maximising cognitive benefits across different populations and age groups. The use of consistent, validated cognitive assessment tools is also warranted to facilitate improved synthesis of findings. In terms of clinical implications, this review provides robust evidence for healthcare practitioners to confidently recommend exercise as an effective intervention for enhancing general cognition, memory and executive function in patients of all ages and health statuses. Exercise prescriptions can be individualised based on patient preferences and abilities, as cognitive gains were observed across various exercise types, intensities, frequencies and durations. Exergaming and mind-body exercises like yoga and Tai Chi may particularly benefit general cognition and memory, respectively. Importantly, even light-intensity exercise can confer substantial cognitive benefits, rendering it an accessible option for diverse populations. Overall, the integration of exercise recommendations into standard clinical care is warranted to optimise cognitive function and holistic health across the lifespan. While supporting the promotion of exercise for cognitive enhancement, this review underscores the need for higher-quality research to further refine tailored exercise prescriptions.
Strengths and limitations
A key strength of our study is that it is the first umbrella review to assess the impact of a wide array of exercise modalities on cognitive function across all age groups, encompassing both general and specific clinical populations. Our methodology was stringent, complying with the PRISMA 2020 and AMSTAR-2 guidelines and involved a search of 11 databases. The vast number of included studies enabled us to perform detailed subgroup analyses to discern the effects across different ages, health conditions and exercise types.
This study is not without limitations. First, the tools used to assess cognitive function varied substantially across and within the included studies. This variability may influence the consistency of the observed results, impacting the final effect sizes reported. Second, it is important to note that many cognitive tests were designed primarily to identify impairments, rather than to differentiate performance among healthy adults, leading to ceiling effects that limit their sensitivity within non-impaired populations. There was also variability in cognitive assessment tools used across studies. Some meta-analyses combined data from studies that employed different cognitive tests, which may measure distinct cognitive domains, introducing heterogeneity into pooled estimates. Another limitation is the poor methodological quality of most reviews, as highlighted by the critically low AMSTAR-2 scores for 71% of the included reviews. This raises concerns about potential biases and lack of transparency in the systematic reviews and meta-analyses included. It is worth noting that the AMSTAR-2 scores of the included reviews do not necessarily imply that the RCTs within those reviews were also of poor quality. Importantly, sensitivity analyses indicated that the exclusion of lower-quality studies did not significantly alter the direction or significance of the pooled effects, suggesting that our overall findings are robust. Another limitation of the current evidence is the lack of studies specifically examining the effects of exercise on cognition in healthy middle-aged adults, compounded by the use of cognitive assessment tools like the MMSE, MoCA and ADAS-Cog, which are designed to detect cognitive impairment rather than subtle differences in healthy individuals. This can lead to ceiling effects, masking the true impact of exercise. Furthermore, many studies combine data from middle-aged and older adults or focus on clinical populations, making it difficult to isolate the effects of exercise on cognition in healthy middle-aged individuals.
Conclusions
Our comprehensive umbrella review synthesises the current evidence on the cognitive benefits of exercise, highlighting its positive effects on general cognition, memory and executive function across diverse populations and exercise modalities. Importantly, these findings suggest that clinicians and public health practitioners can confidently recommend regular physical activity as a strategy to support cognitive health across the lifespan. Most forms of exercise appear effective, including light-intensity activities, exergaming and mind-body practices such as yoga and Tai Chi, making exercise an accessible and versatile intervention. While the evidence base highlights the need for further high-quality studies to confirm and refine these findings, this review provides strong support for the role of exercise in promoting cognitive function and overall health.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article and its supplementary information files.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
X @bensinghphd, @_HunterBennett_, @jacintabrinsley, @CLEkegren
Contributors BS led the project, drafted the manuscript and is the guarantor. BS, HB, AM, DD, RC, TF, JB, KS, EE, CEMS, JMP, CG, CLE, AS, KIE and CM drafted the initial study protocol. BS, HB, AM, DD, RC, TF, JB, KS, EE, CEMS, JMP, CG and CLE conducted screening, extraction and risk of bias assessment. BS conducted statistical analyses. CM, AS, and KIE provided supervision and mentorship. All authors reviewed and approved the final manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This project received no specific funding.DD is supported by an Australian Research Council Discovery Early Career Award (DE230101174) and by the Centre of Research Excellence in Driving Global Investment in Adolescent Health funded by NHMRC APP1171981.AM is supported by the Centre of Research Excellence in Driving Global Investment in Adolescent Health funded by NHMRC APP1171981.CM is supported by a Medical Research Future Fund Emerging Leader Grant (GNT1193862).AES is supported by a Henry Brodaty Dementia Australia Research Foundation mid-career fellowship.The other authors received no additional funding.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.